
Why 640nm Is the Gold Standard
Wavelength for Red Light Therapy:
The Mitochondrial Physics Explained
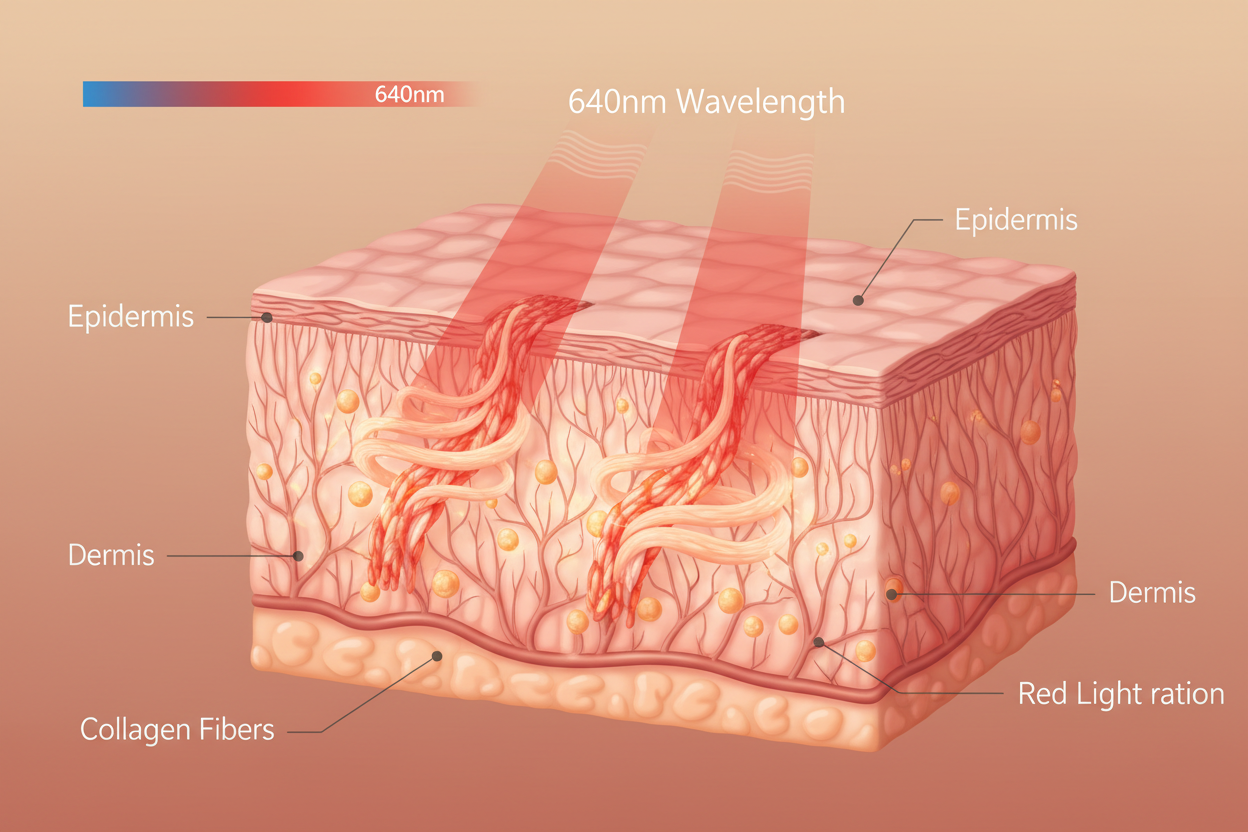
Not all red light is created equal. A 630nm LED and a 640nm LED look nearly identical to your eyes — but at the molecular level, the 10nm difference changes how efficiently they activate the mitochondrial enzyme that drives collagen, anti-aging, and tissue repair. This is the physics of why 640nm specifically is the globally validated wavelength for photobiomodulation.
640nm sits at the absorption peak of Cytochrome c Oxidase — the terminal enzyme of the mitochondrial electron transport chain. When CCO absorbs a 640nm photon, it displaces inhibitory nitric oxide, unblocking ATP synthesis and producing a 200–400% energy surge. Combined with minimal Rayleigh scattering (enabling 5–10mm dermal penetration) and its position in the therapeutic optical window (600–900nm), 640nm is the most clinically validated wavelength for collagen, anti-aging, acne, and pain treatment.
Wavelengths are measured in nanometers. A nanometer is one billionth of a metre. The difference between 630nm and 640nm is 10 billionths of a metre — completely invisible to the naked eye, and to almost every instrument a consumer would use to evaluate an LED device. Yet this 10nm difference changes how efficiently the light activates the molecular gateway to cellular repair. Understanding why requires understanding one specific enzyme.
The Molecular Target — Why Cytochrome c Oxidase Changes Everything
Photobiomodulation does not work on all cells equally, and it does not work through all wavelengths equally. It works because one specific enzyme — Cytochrome c Oxidase (CCO), Complex IV of the mitochondrial electron transport chain — absorbs specific wavelengths of light and changes its behaviour as a result.
CCO is the terminal enzyme that transfers electrons to oxygen, completing the synthesis of ATP. In healthy, young cells it operates efficiently. In stressed, aged, or inflamed cells, nitric oxide (NO) accumulates and competitively inhibits CCO — blocking the electron transport chain and reducing ATP output. This is a primary driver of the cellular energy deficit underlying aging, inflammation, and slow tissue repair.
When CCO absorbs photons at its specific wavelength peaks, those photons displace the inhibitory NO — restoring electron transport chain function and producing an immediate ATP surge. The question is: at which wavelength is this displacement most efficient?
Three Biological Reasons 640nm Outperforms Adjacent Wavelengths
Mitochondrial Activation — Peak CCO Absorption
640nm sits at the red-range absorption peak of Cytochrome c Oxidase. The enzyme's chromophore components (haem a3 and CuB) most efficiently absorb photons at this wavelength. Each absorbed photon displaces inhibitory nitric oxide from the enzyme, restoring electron transport chain function. The result is a 200–400% increase in ATP production — the energy surge that powers collagen synthesis, cellular repair, and inflammation resolution.
Optimal Dermal Penetration — 5 to 10mm
640nm penetrates tissue to 5–10mm — deep enough to reach dermal fibroblasts that produce collagen and elastin, but shallow enough to concentrate photonic energy at this target layer rather than dispersing it into deeper structures. Blue light (465nm) never reaches the dermis. Near-infrared (880nm) passes through it entirely to reach deeper tissue. 640nm deposits energy specifically where fibroblasts are densely concentrated.
Anti-Inflammatory Cytokine Modulation
640nm activates a secondary mechanism independent of ATP: it downregulates pro-inflammatory cytokines — specifically TNF-alpha and Interleukin-6 (IL-6) — by modulating nuclear factor kappa-B (NF-κB) signalling. This shifts tissue from the inflammatory phase to the proliferative repair phase. Combined with the ATP surge, these two simultaneous mechanisms are why 640nm is clinically effective for both anti-aging and inflammatory conditions.
Penetration Depth Comparison — Blue, Red, and Near-Infrared
Each wavelength penetrates tissue to a different depth determined by its optical scattering and absorption properties in biological tissue. Understanding these depths makes it clear why different wavelengths are used for different clinical indications.
640nm vs 630nm vs 660nm — Does the Difference Matter?
The most common question from consumers evaluating LED devices: if 630nm, 640nm, and 660nm all look the same red colour, does the 10–20nm difference actually matter clinically?
| Wavelength | CCO Activation | Tissue Penetration | Clinical Use | Notes |
|---|---|---|---|---|
| 620nm | Moderate | 3–5mm | Superficial skin | Below the CCO absorption peak |
| 630nm | Good | 4–7mm | Anti-aging, skin | Near peak — slightly sub-optimal |
| 640nm ★ | Optimal | 5–10mm | Anti-aging, acne, wound healing | CCO absorption peak — FDA-cleared Celluma spec |
| 650nm | Very good | 5–10mm | Anti-aging, skin | Within clinical range, used in many RCTs |
| 660nm | Good | 5–10mm | Anti-aging, muscle | Commonly used, slightly past peak |
| 700nm | Reduced | 7–12mm | Deeper tissue | Between red and NIR — transitional |
The Physics of Deep Penetration — Rayleigh Scattering
Why does 640nm penetrate 5–10mm when 465nm barely reaches 2mm? The answer is Rayleigh scattering — the optical phenomenon governing how light interacts with particles smaller than its wavelength in tissue.
Scattering intensity is inversely proportional to the fourth power of wavelength
λ⁴ means that doubling the wavelength reduces scattering by a factor of 16. 640nm is approximately 1.38× the wavelength of 465nm — meaning 640nm experiences (1.38)⁴ ≈ 3.6× less scattering than 465nm blue light. Blue light scatters rapidly in the superficial tissue layers and never reaches the dermis. 640nm travels deeper with its energy substantially intact, concentrating therapeutic photon flux at the fibroblast-dense dermis.
Celluma Devices Using 640nm + 880nm — FDA-Cleared
Frequently Asked Questions
640nm sits at the absorption peak of Cytochrome c Oxidase — the mitochondrial enzyme that drives ATP synthesis. When CCO absorbs a 640nm photon, it displaces inhibitory nitric oxide and restores electron transport chain function, producing a 200–400% ATP surge. Combined with minimal Rayleigh scattering (5–10mm dermal penetration) and its position in the 600–900nm therapeutic optical window, no other single red wavelength activates CCO as efficiently.
640nm penetrates 5–10mm below the skin surface, reaching the dermis where fibroblasts produce collagen and elastin. Compare: 465nm blue light penetrates only 1–2mm (epidermis — for acne bacteria). 880nm near-infrared penetrates 10–30mm+ (muscle, joints — for pain and deep inflammation). 640nm is specifically optimised for the dermal fibroblast layer that no topical skincare product can reach.
All three are within the therapeutic window and produce clinically meaningful photobiomodulation. 640nm sits closest to the CCO absorption peak — producing slightly more efficient enzyme activation per photon at equivalent irradiance. In practice, the difference is not dramatic (all three are used in clinical research). More important than ±10nm is the device's irradiance (mW/cm²), zero-gap panel contact, and 30-minute session duration.
Yes — 640nm red light downregulates TNF-alpha and IL-6 (pro-inflammatory cytokines) by modulating NF-κB signalling. This anti-inflammatory effect operates simultaneously with the ATP mechanism — both pathways activate in the same 30-minute session. This is why 640nm treats both anti-aging conditions (collagen synthesis) and inflammatory conditions (acne, pain) through the same device mode.
CCO (Complex IV) is the final enzyme in the mitochondrial electron transport chain — it transfers electrons to oxygen to complete ATP synthesis. In aged or stressed cells, nitric oxide accumulates and competitively blocks CCO, reducing ATP output. 640nm photons are absorbed by CCO's chromophore metal centres (haem a3, CuB), displacing the inhibitory NO and restoring full electron transport chain function — producing an immediate ATP surge that powers cellular repair.
Biological chromophores like CCO have specific absorption spectra. Light 20–30nm outside the absorption peak produces significantly less enzyme activation at the same irradiance — equivalent to using a key that almost fits the lock. Consumer devices often use broad-spectrum LEDs across 620–700nm. Medical-grade devices specify wavelength to ±5nm. Within the therapeutic window, 640nm produces greater CCO activation than 620nm at identical power output.
Rayleigh scattering is the deflection of light by tissue particles. Scattering intensity ∝ 1/λ⁴ — meaning longer wavelengths scatter exponentially less. Blue light (465nm) scatters approximately 3–4× more than 640nm red, explaining why blue light stays in the epidermis at 1–2mm while red light travels 5–10mm to the dermis. Without Rayleigh scattering reduction, red light could not reach the fibroblasts responsible for collagen production.
Yes — Celluma delivers 640nm (red) and 880nm (near-infrared) simultaneously. 640nm targets CCO in the dermis (4–6mm) for collagen, anti-aging, and inflammation. 880nm penetrates deeper (6–10mm+) for pain, muscle recovery, and systemic anti-inflammatory effects. This dual-wavelength simultaneous delivery is why Celluma holds FDA Class II Clearance for multiple clinical indications from a single device.
Not All Red Light
Is Red Light Therapy.
Celluma delivers clinically calibrated 640nm at verified irradiance — the exact wavelength and power density that activates Cytochrome c Oxidase for collagen, anti-aging, and repair.

{kind=link}
Leave a comment
This site is protected by hCaptcha and the hCaptcha Privacy Policy and Terms of Service apply.