
Fungal acne and bacterial acne look almost identical — but need completely opposite treatments. Fungal acne (Malassezia folliculitis) is caused by yeast, not bacteria, and requires antifungal treatment. Antibacterial acne treatments don't work and often make it worse. The key clues: fungal acne is uniformly small, itchy, and resistant to standard acne products.
The Critical Difference: Bacteria vs Yeast
Why Singapore's Climate Increases Fungal Acne Risk
Malassezia yeast thrives in warm, humid environments — which describes Singapore's year-round tropical climate precisely. Add the fact that Singapore's dermatologists frequently prescribe topical and oral antibiotics for acne (which kill the bacterial competition keeping Malassezia in check), and the result is a higher prevalence of Malassezia folliculitis than is seen in temperate countries. Many Singaporeans are unknowingly treating fungal acne with antibacterial products, worsening the underlying yeast overgrowth.
How to Tell Which You Have: The Diagnostic Test
Note on LED therapy and fungal acne: Blue LED therapy at 465nm targets P. acnes bacterial porphyrins — it does not have direct antifungal effects on Malassezia. If you have confirmed or suspected fungal acne, the primary treatment is antifungal. If you have both bacterial and fungal acne simultaneously, blue LED therapy can address the bacterial component while antifungal treatment addresses the yeast.
Questions & Answers
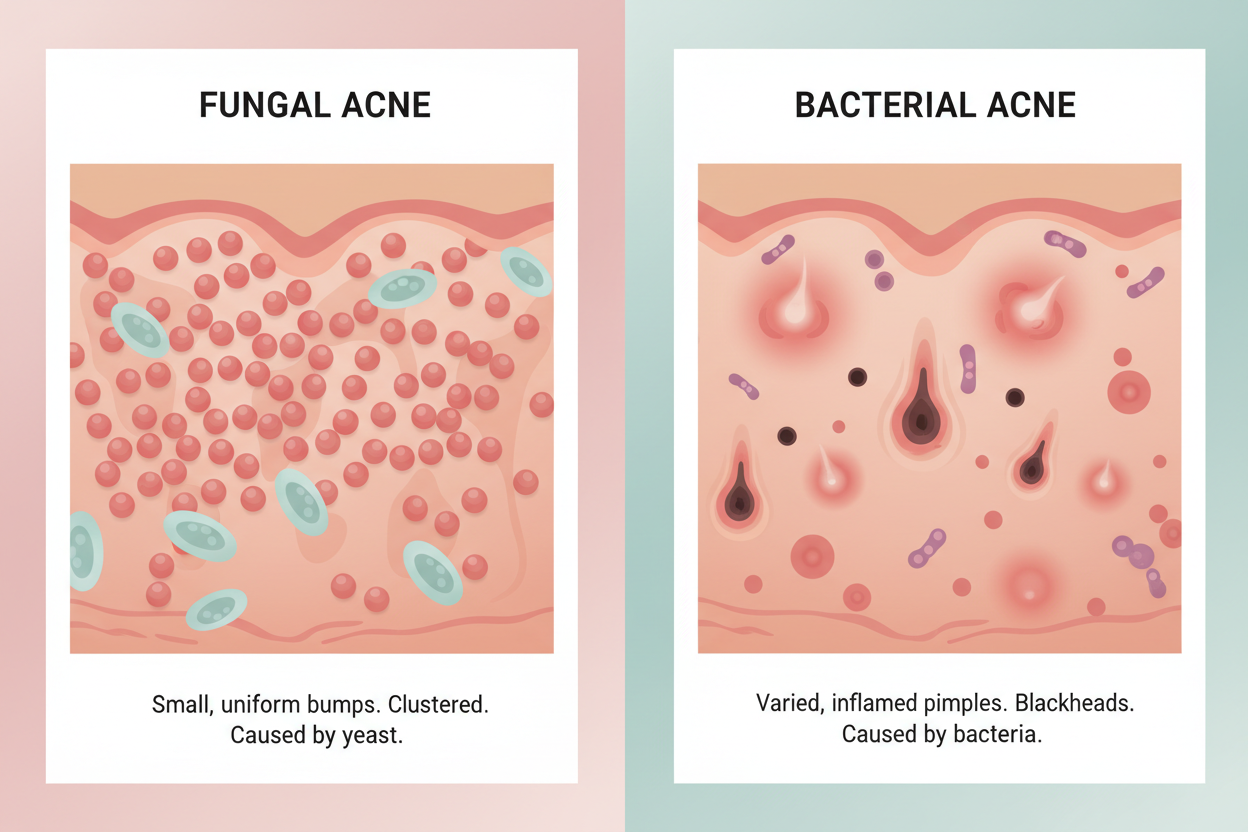
Fungal acne (Pityrosporum folliculitis or Malassezia folliculitis) is not actually acne — it is a yeast infection (Malassezia species) inside hair follicles. Unlike bacterial acne caused by P. acnes bacteria, fungal acne is caused by overgrowth of a naturally occurring yeast. It appears as uniform small (1-2mm) flesh-coloured to whitehead bumps, often itchy, typically on the forehead, chest, back, and upper arms. It does not respond to antibacterial acne treatments and worsens with heavy moisturisers and oils that feed the yeast.
Key differentiators: Fungal acne lesions are (1) very uniform in size (all about 1-2mm, no large nodules); (2) often itchy; (3) concentrated in the same size clusters; (4) resistant to or worsening with standard acne treatments; (5) often appear or worsen after antibiotics (which kill the bacterial competition that keeps Malassezia in check) or after starting heavy moisturisers/oils. Bacterial acne has varied lesion sizes (blackheads, whiteheads, papules, nodules), is usually not itchy, and responds to antibacterial treatments.
Blue LED at 465nm targets P. acnes bacterial porphyrins specifically — it is not effective against Malassezia yeast, which has a different biochemistry. However, if you have both fungal and bacterial acne simultaneously (common, as antibiotics used for bacterial acne can trigger Malassezia overgrowth), LED therapy addresses the bacterial component while antifungal treatment addresses the fungal component. A dermatologist can confirm the diagnosis with a skin scraping test and prescribe the appropriate antifungal.
Common triggers: (1) Antibiotics — kill bacterial competition that normally keeps Malassezia populations in check; (2) Heavy skincare oils and fatty acid-rich products (e.g., coconut oil, argan oil, squalane) — Malassezia feeds on C11-C24 fatty acids; (3) Hot, humid climates — Singapore's year-round tropical heat is ideal for Malassezia overgrowth; (4) Excessive sweating without prompt showering; (5) Immunosuppression; (6) Tight occlusive clothing. Singapore's climate makes fungal acne significantly more prevalent than in temperate countries.
Fungal acne is treated with antifungal agents, not antibacterial treatments: (1) Ketoconazole 2% shampoo used as a face/body wash (leave on 3-5 minutes before rinsing) — highly effective; (2) Zinc pyrithione-containing washes; (3) Selenium sulphide shampoo; (4) Oral antifungals (fluconazole, itraconazole) for severe or resistant cases — prescription required. Crucially, eliminate fatty acid-rich skincare products (coconut oil, olive oil, vitamin E) that feed the yeast. Switch to Malassezia-safe moisturisers.
Yes — and this is common, particularly after antibiotic treatment for bacterial acne. The antibiotics clear P. acnes but disrupt the microbial balance, allowing Malassezia yeast to overgrow. The result is persistent 'acne' that doesn't respond to continued antibacterial treatment. If your acne worsens or changes character (becomes more uniform, itchy) during or after antibiotic treatment, fungal overgrowth is a strong possibility. A dermatologist consultation for proper diagnosis is the appropriate next step.

{kind=link}
留言
此網站已受到 hCaptcha 保護,且適用 hCaptcha 隱私政策以及服務條款。